Keratoconus gets worse over time if left untreated. Doctors divide it into stages to track how far it has progressed. Knowing your stage helps your doctor choose the right treatment for you.
The most common staging system is called the Amsler-Krumeich system. It divides keratoconus into four stages based on corneal shape and thickness. Doctors use special tests and imaging tools to find your stage accurately.
How Doctors Stage Keratoconus?
Several tools help doctors measure the stage of keratoconus. Each tool looks at a different part of the cornea. Together, they give a full picture of the condition.
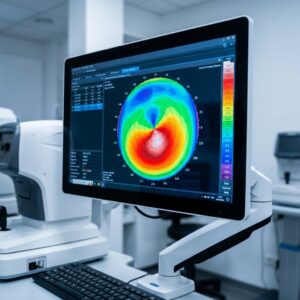
Corneal Topography
This test maps the surface of the cornea in detail. It shows steepening, irregularity, and early changes in corneal shape. It is one of the most important tools for staging keratoconus.
Pachymetry
Pachymetry measures how thick the cornea is. A thinner cornea signals a more advanced stage of keratoconus. This test helps doctors track thinning over time.
Keratometry
Keratometry measures the curvature of the cornea. Steeper curvature means the condition has progressed further. Doctors use these readings to classify the severity of the disease.
Corneal Tomography and OCT
These tools create detailed 3D scans of the entire cornea. They show both the front and back surfaces of the corneal tissue. This data helps doctors plan the most effective treatment.
The Four Stages of Keratoconus
Mild Keratoconus
In the mild stage, changes in the cornea are very subtle. The cornea begins to steepen slightly, but there is little or no scarring. Vision may be mildly blurry, especially at night or in low light.
Signs of the mild stage
Patients often notice minor astigmatism or slight nearsightedness. Glasses or soft contact lenses may still correct vision at this stage. Many people do not even know they have keratoconus this early.
Solution for Mild Keratoconus stage
Rigid gas-permeable (RGP) lenses give sharper vision than soft lenses. Scleral lenses are also a great option, even at this early stage. Regular eye exams with corneal mapping are key to catching changes early.
Moderate Keratoconus
At this stage, the cornea steepens more and scarring may begin. Vision distortion gets worse and glasses can no longer fully help. Glare, halos, and sensitivity to light become more noticeable.
Solution for the Moderate Keratoconus stage
- RGP lenses or hybrid lenses are commonly used at this stage. Hybrid lenses have a rigid center for sharp vision and a soft ring for comfort. Scleral lenses are also an excellent option for clear, stable vision.
- Corneal cross-linking (CXL) is often recommended at this stage. CXL uses UV light and special eye drops to strengthen the cornea. It stops the cornea from thinning and bulging further.
- Intacs may also be used to help reshape the cornea. These are small ring implants placed inside the corneal tissue. They reduce the cone shape and can improve how lenses fit.
Preventive measures
Follow-up visits every three to six months are important at this stage. Your doctor will check for changes and adjust your lens fit as needed. Early action at this stage can prevent the condition from getting worse.
Advanced Keratoconus
Advanced keratoconus brings significant thinning and visible corneal scarring. The cornea bulges more and vision becomes severely distorted. Reading, driving, and screen use all become very difficult.
Effective Treatments for Advanced Keratoconus
Glasses are no longer effective at this stage. Custom scleral lenses are the best option for vision correction. They vault over the damaged cornea and give stable, comfortable sight.
Cross-linking may still be performed if the condition is still progressing. Advanced imaging helps doctors monitor both the front and back of the cornea. Corneal hydrops, a sudden fluid buildup in the cornea, may also need treatment.
Signs and Symptoms of Advanced Keratoconus
Patients at this stage often feel eye strain and frequent headaches. The vision changes can happen quickly and affect everyday confidence. Timely care and a good lens fit make a major difference in daily life.
Severe Keratoconus
In the severe stage, the cornea is extremely thin and heavily scarred. Vision is very poor and most contact lenses are hard to tolerate.
Effective Treatment Options for Severe Keratoconus
A corneal transplant is often the only option left at this point. There are two main types of corneal transplant.
- A full-thickness transplant replaces the entire cornea.
- A partial transplant preserves the inner layers and lowers rejection risk.
After a transplant, scleral lenses are often still needed. They help correct any remaining irregularities in the new cornea.
Michigan Contact Lens specializes in fitting scleral lenses post-transplant.
The Belin ABCD Staging System
The Belin ABCD system is a newer, more detailed way to stage keratoconus. It uses four measurements to give a complete picture of the disease. Many doctors now use it alongside the Amsler-Krumeich system.
A — Anterior Curvature
This measures the steepness of the front surface of the cornea. Steeper readings suggest more advanced keratoconus progression.
B — Back Curvature
This measures the curvature of the back surface of the cornea. Changes here often appear before the front surface is affected.
C — Corneal Thickness
This tracks how thin the cornea has become over time. Thinning is one of the clearest signs that keratoconus is progressing.
D — Visual Function
This measures how well the patient can see with the best correction possible. It shows how much the condition is affecting real-world vision.
How Does Keratoconus Progress?
The speed of progression is different for every patient. It tends to move faster in younger people and slower in older adults. Most patients see the biggest changes in the first 15 to 20 years.
The condition usually stabilizes around age 40 to 45. Some patients continue to see small changes even after this age. Regular monitoring is the only way to know what is happening in your eyes.
Each eye can progress at a different rate, too. Your doctor will monitor each eye separately at every visit. This helps catch changes early and adjust your treatment plan fast.
How AI Is Changing Keratoconus Diagnosis
Artificial intelligence is now being used in keratoconus eye care. AI tools analyze corneal images faster and more accurately than ever before. They can detect early changes that are too subtle for traditional methods.
AI-Powered Corneal Imaging
AI scans corneal topography and OCT images for early warning signs. It spots small shifts in corneal shape and thickness before symptoms appear. This leads to earlier diagnosis and faster treatment decisions.
Predicting Disease Progression
AI can compare current scans with past data to predict future changes. It helps doctors know when to act before vision gets worse. This is especially useful for younger patients with fast-moving disease.
Personalized Treatment Planning
AI reviews a patient’s full history and eye data to suggest the best options. It can identify who would benefit most from cross-linking or scleral lenses. This leads to more targeted and effective care for each patient.
Remote Monitoring via Telemedicine
AI tools now work with remote platforms for patients far from clinics. Patients can submit eye scans and get results without an in-person visit. This expands access to expert keratoconus care across wider areas.
Conclusion
Keratoconus is a progressive condition, but it can be managed well. Knowing your stage gives you and your doctor a clear path forward. Early detection and the right treatment protect your vision long term.
Whether you are in stage one or stage four, help is available. Michigan Contact Lens specializes in every stage of keratoconus care. Call us today to schedule a full corneal evaluation
Frequently Asked Questions
Can keratoconus progress differently in each eye?
Yes, the condition can progress at different rates in each eye, requiring individualized monitoring and lens fitting.
Do contact lenses stop keratoconus progression?
No, contact lenses improve vision but do not prevent progression. Corneal cross-linking is the primary intervention to stabilize the cornea.
At what age does keratoconus stop progressing?
Most patients stabilize around age 40–45, though minor progression may occur later in some cases
How can I know my stage of keratoconus?
Through comprehensive eye exams, including corneal topography, pachymetry, keratometry, and slit-lamp examination.
Can early intervention prevent surgery later?
Yes, early detection and treatments like cross-linking or specialized lenses often reduce or delay the need for a corneal transplant.
Related: Explore your full range of keratoconus treatment in Michigan — from corneal cross-linking to custom specialty lenses.