If you’ve been told you have keratoconus in one eye, here’s what the research consistently shows: truly one-eyed keratoconus is rare. In most “unilateral” cases, sensitive corneal imaging finds early changes in the other eye too — the disease is almost always in both eyes, just dramatically asymmetric. That changes how your “good” eye should be treated: not as healthy, but as watched.
Why one eye gets so far ahead
Keratoconus is famously asymmetric — one cornea can be steepening for years while the other barely moves. One well-documented contributor: habits. People tend to rub one eye more than the other (the side you sleep on, your dominant hand, the eye that itches most), and rubbing is the strongest behavioral driver of progression. Whatever the mechanism, the gap between eyes can be so large that the milder eye passes a routine exam while the worse eye is sending you to specialists with ghosting and blur.
What this means for your “good” eye
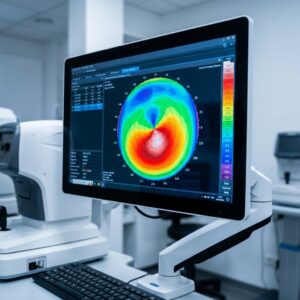
Both eyes get mapped — always. Corneal topography and profilometry catch the subtle early steepening a chart-based exam misses, and a baseline map of the better eye is the reference that makes any future change obvious. If the better eye shows early disease and is progressing, cross-linking can stop it while that eye still sees well — the single best outcome in keratoconus care is the eye that never gets worse. Protect both eyes the same way: no rubbing, allergies and dryness treated, stage checked on schedule.
Treating the affected eye
The worse eye follows the standard playbook: stop progression if it’s moving, and correct the vision the cone has distorted. For asymmetric patients, a scleral lens on the affected eye often restores the sharp, stable image that lets both eyes work together again — many patients don’t realize how much depth perception and comfort they lost until binocular vision comes back.
One eye worse ≠ one eye safe
The practical summary: treat the diagnosis as bilateral until years of stable maps prove otherwise. The patients who regret their care are rarely the ones who watched the good eye too closely.
Can you have keratoconus in only one eye?
Truly unilateral keratoconus is rare. In most cases diagnosed in one eye, sensitive corneal imaging reveals early changes in the other eye as well — the disease is bilateral but highly asymmetric.
Will my other eye get keratoconus too?
The other eye often already shows subtle early changes on imaging. Regular mapping of both eyes catches any progression early, when cross-linking can stop it before vision is affected.
Why is my keratoconus so much worse in one eye?
Keratoconus is naturally asymmetric, and habits amplify the gap — people typically rub one eye more than the other, and rubbing is the strongest behavioral driver of progression.
Diagnosed in one eye? Let’s map both and build the plan. Dr. Shira Kresch monitors and fits keratoconus patients from across Metro Detroit at our Southfield office — your first specialty consultation is free. Book online or call (248) 545-2800.