If you have Sjogren’s Syndrome, you already know that eye drops offer only minutes of relief. Soft contact lenses make things worse. And blinking constantly just to get through a workday has become exhausting.
You are not imagining it. Sjogren ‘s-related dry eye is among the most difficult forms of dry eye disease to treat. Standard options fall short because the root problem is systemic; your immune system has damaged the very glands that produce tears.
Scleral lenses work differently. They do not rely on your tear glands at all. Instead, they create a sealed reservoir of moisture that sits directly over your eye for hours. For many Sjogren’s patients, this is the first treatment that provides real, lasting comfort during the day.
This guide explains how scleral lenses work, what the fitting process looks like, and what to expect in 2026.
What Is Sjogren’s Syndrome?
Sjogren’s Syndrome is a chronic autoimmune disorder. The immune system mistakenly attacks the body’s moisture-producing glands, particularly the lacrimal glands in the eyes and the salivary glands in the mouth.
The most common symptoms are:
- Dry eyes: Reduced tear production leads to burning, stinging, and light sensitivity.
- Dry mouth: Saliva loss causes difficulty swallowing, speaking, and tasting.
- Joint pain and fatigue: The condition affects tissues throughout the body, not just the eyes.
Sjogren’s affects approximately four million Americans. It is most common in women over 40, though it can occur at any age. Of all its symptoms, chronic dry eye tends to have the greatest impact on daily function. Left unmanaged, severe dry eye can cause corneal damage over time.
How Scleral Lenses Work for Sjogren’s Syndrome
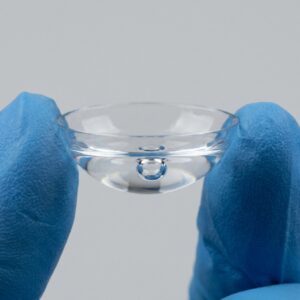
Scleral lenses are large-diameter, rigid gas-permeable contact lenses. They vault completely over the cornea and rest on the white part of the eye, the sclera, rather than on the corneal surface itself.
This design creates a fluid-filled chamber between the lens and the eye. That chamber is filled with preservative-free saline before insertion. Throughout the day, it serves as a continuous source of moisture. Your tear glands do not need to contribute anything.
Think of it as a tiny aquarium for your eye, sealed, stable, and consistently hydrated.
Why does this matter for Sjogren’s patients?
Soft lenses draw moisture from the eye surface. They depend on your tear film to stay comfortable. Because Sjogren depletes that tear film, soft lenses typically increase dryness and irritation. Scleral lenses bypass that problem entirely.
Clinical studies consistently report that the majority of patients with severe aqueous-deficient dry eye — the type common in Sjogren’s — experience significant symptom improvement after switching to scleral lenses.
Scleral Lenses vs. Soft Lenses
| Feature | Soft Lenses | Scleral Lenses |
| Moisture retention | Wicks moisture away from the eye | Holds a sealed reservoir of saline |
| Comfort for dry eye | Poor — worsens dryness | Excellent — designed for severe dry eye |
| Environmental protection | None | Shields against wind, dust, and allergens |
| Fit | Standardized | Custom-fitted to your eye shape |
| Corneal contact | Rests directly on the cornea | Vaults over the cornea entirely |
For many patients with Sjogren’s Syndrome, scleral lenses succeed where soft lenses and drops fall short — because they address the underlying mechanism of the condition rather than just its symptoms. They work best as part of a broader dry-eye management plan, alongside the adjunct therapies described below.
Benefits of Scleral Lenses for Sjogren’s Dry Eye
Continuous Hydration
The saline reservoir does not evaporate quickly. It provides steady moisture to the ocular surface for many hours. Patients who previously applied eye drops every 30 minutes often find they can go through a full workday without interruption.
Protection from Environmental Triggers
Wind, air conditioning, and allergens significantly worsen Sjogren’s dry eye. Scleral lenses create a physical barrier. The eye sits behind the lens rather than being exposed to the environment. This alone can reduce flare-ups during outdoor activity or air travel.
Improved Vision Stability
Dry eyes cause the tear film to break up rapidly. This creates fluctuating, blurry vision — a symptom many Sjogren’s patients describe as among the most disruptive. Scleral lenses stabilize the refracting surface of the eye. Vision remains clearer and more consistent throughout the day.
Reduced Corneal Damage Risk
Chronic dryness causes micro-abrasions on the corneal surface. Over the years, this can lead to corneal scarring. The fluid reservoir in a scleral lens protects the cornea and allows the surface to heal, particularly in patients who present with existing ocular surface damage.
Scleral Lenses Fitting Process
Fitting scleral lenses is a specialized process. It requires an optometrist or ophthalmologist with specific training in specialty contact lenses. Not every eye care provider offers this service; it is worth seeking out a clinic that lists scleral lens fitting as a clinical focus.
The Fitting Process
- Comprehensive evaluation: Your provider will assess your corneal shape with corneal topography, measure your ocular surface, and evaluate the quality of your tear film. They will also review your current medications, as some Sjogren’s treatments affect lens compatibility.
- Trial lens fitting: A diagnostic lens is placed on the eye. Your provider assesses the vault height, the space between the back of the lens and the corneal surface. Too little vault causes the lens to touch the cornea. Too much vault creates excessive fogging.
- Custom lens order: Once the fit is refined, a lens is ordered to your exact parameters. This typically takes one to two weeks.
- Dispensing and training: Your provider teaches you how to insert, remove, fill, and clean your lenses. This step takes time. Do not rush it.
- Follow-up appointments: Sjogren’s can alter corneal shape over time. Regular follow-ups, typically every six to twelve months — ensure the fit remains optimal.
Key Variables in the Fit
- Vault height: The most critical parameter for Sjogren’s patients. A higher vault keeps the reservoir from compressing against the cornea.
- Landing zone: The area where the lens meets the sclera must be smooth and pressure-free.
- Sagittal depth: This determines how much fluid the reservoir holds. Patients with severe dry eye often benefit from a deeper sag.
Care for Your Scleral Lenses
Proper care protects both the lens and your eye. Follow these guidelines consistently.
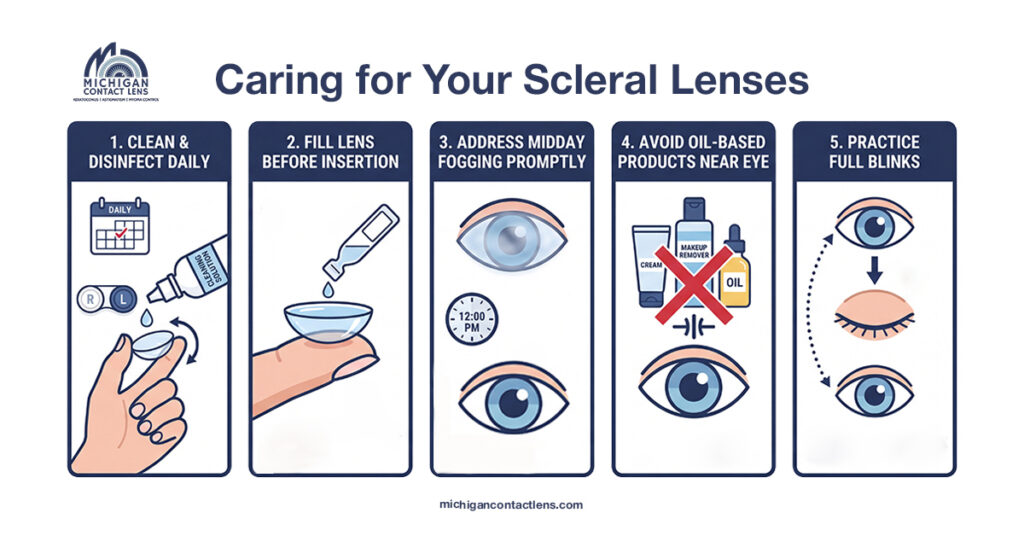
Clean and disinfect daily
Use only preservative-free saline or the specific solution your provider recommends. Preserved solutions contain chemicals that accumulate on the lens surface and cause ocular surface irritation, a serious concern for Sjogren’s patients whose corneas are already compromised. Skipping even one cleaning session allows protein and lipid deposits to build up, leading to fogging, discomfort, and reduced lens life.
Fill the lens before insertion
Leave no air bubbles in the reservoir when you fill the bowl of the lens with saline. Bubbles create immediate fogging and generate uneven pressure points against the corneal surface, which can cause pain and temporary vision distortion. Tilt the filled lens carefully during insertion and work in front of a mirror to confirm the reservoir stays intact as the lens sits on the eye.
Address midday fogging promptly
Fogging occurs when proteins or lipids from the ocular surface migrate into the saline reservoir and cloud it over time. Remove the lens, rinse it thoroughly with fresh preservative-free saline, refill the bowl completely, and reinsert. If fogging becomes frequent rather than occasional, contact your provider; it often signals a meaningful change in fit, tear chemistry, or lens surface condition that needs professional attention.
Avoid oil-based products near the eye
Oil-based moisturizers, makeup removers, and certain medicated eye drops leave a residue on the lens surface that prevents the saline from spreading evenly, a condition called surface non-wetting. This causes dry spots on the lens within minutes of insertion, defeating the purpose of wearing the lens at all. Apply all oil-based products only after lens removal and wash your hands thoroughly with an oil-free soap before handling your lenses each morning.
Practice full blinks
Incomplete blinking is extremely common during screen use, reading, and concentrated focus tasks — and it reduces the contact between the eyelid and the lens surface that keeps the outer layer of the lens hydrated. Over time, partial blinks accelerate fogging and cause the outer lens surface to feel dry and uncomfortable even though the reservoir beneath remains full. Make a conscious habit of blinking slowly and fully every few minutes, especially during long work sessions, to keep the lens surface performing properly.
Holistic Approaches to Managing Sjogren’s Dry Eye Beyond Scleral Lenses
Scleral lenses manage symptoms effectively. They do not treat the underlying disease. Combining lens wear with these adjunct therapies produces the best outcomes.
Intense Pulsed Light (IPL) Therapy
IPL targets Meibomian Gland Dysfunction, which often accompanies Sjogren’s. The glands that produce the oily layer of the tear film become blocked or dysfunctional. IPL stimulates gland activity and improves tear film quality. It does not conflict with scleral lens wear.
Punctal Plugs
These are tiny silicone devices inserted into the tear drain openings of the eyelids. They slow tear drainage and help retain whatever moisture the eye does produce. For Sjogren’s patients, punctal plugs work well alongside scleral lenses.
Prescription Eye Drops
Cyclosporine drops (Restasis, Cequa) and lifitegrast (Xiidra) reduce ocular surface inflammation. They are not a substitute for scleral lenses, but they address the inflammatory component of Sjogren’s dry eye at a cellular level.
Eyelid Hygiene
Warm compresses applied to closed eyelids for five to ten minutes daily soften blocked Meibomian gland secretions. Follow with a gentle lid scrub. This routine reduces lid margin inflammation and improves the quality of any natural tear production that remains.
Oral Secretagogues
In some cases, physicians prescribe pilocarpine or cevimeline to stimulate residual gland activity. These medications modestly increase tear and saliva production in patients who retain some gland function.
Cost and Insurance Coverage
Scleral lens pricing reflects a custom medical fitting rather than an off-the-shelf product — the investment depends on the complexity of your eyes, the lens design your case requires, and the follow-up care built into your fitting. Because every Sjogren’s case is different, the exact figure is something your specialist will walk through with you up front, before you commit to anything.
Many medical insurance plans reimburse a portion of medically necessary scleral lens care for documented Sjogren’s Syndrome, even when the practice is out-of-network. At Michigan Contact Lens, we provide a detailed superbill after your visit — an itemized statement with the diagnosis and procedure codes for keratoconjunctivitis sicca and Sjogren’s Syndrome that your insurer needs. You submit it, and reimbursement comes to you based on your out-of-network benefits. HSA/FSA funds and CareCredit also apply.
For the full picture of how reimbursement, superbills, and payment options work, see our Insurance & Payment Options page.
Conclusion
Sjogren’s Syndrome dry eye is severe, progressive, and often resistant to standard treatments. Scleral lenses address the core problem directly. They do not rely on your damaged tear glands. They create an independent moisture source that keeps your ocular surface protected and hydrated from the moment you insert them until you remove them at the end of the day.
If you have been managing with drops, blinking constantly, or avoiding screens and air conditioning to get through the day, scleral lenses are worth a serious conversation with an eye care specialist. Seek a provider who specializes in ocular surface disease and has documented scleral lens fitting experience.
Relief is possible. It just requires the right tool. Dr. Shira Kresch fits scleral lenses for Sjogren’s patients from across Metro Detroit at our Southfield office — your first specialty consultation is free, with no commitment. Book online or call (248) 545-2800.
Frequently Asked Questions
Can I use eye drops while wearing scleral lenses?
Yes, but only preservative-free drops, applied to the outer surface of the lens. Drops with preservatives can degrade the lens material and irritate the ocular surface over time. Ask your provider which drops are compatible with your specific lens material.
How many hours a day can I wear scleral lenses?
Most patients comfortably wear scleral lenses for 12 to 16 hours per day. Your tolerance will depend on fit quality, lens hygiene, and disease severity. Your provider will advise a wear schedule tailored to your case.
Why did fogging suddenly start after months of no problems?
Sudden-onset fogging, after a stable period, usually signals one of three things: a change in corneal shape, a new skincare product or medication affecting tear chemistry, or a lens that needs professional cleaning or replacement. Book an appointment rather than continuing to tolerate it.
How long do scleral lenses last?
With proper care, most scleral lenses last one to three years. Protein deposits and lens warpage are the most common reasons for earlier replacement.
Are scleral lenses safe for long-term wear in Sjogren’s patients?
Yes. Research supports long-term scleral lens wear as safe and effective for aqueous-deficient dry eye. Corneal oxygen transmission is maintained through gas-permeable materials. Regular follow-up appointments catch any issues before they become clinical concerns.
What happens if my Sjogren progresses?
The lens parameters can be updated as the disease progresses. A higher vault or different landing zone profile may be needed. This is one reason ongoing specialist care matters — the fit is not a one-time event.