Still Struggling With Eye Pain After a Bone Marrow Transplant?
If you have been diagnosed with ocular Graft vs. Host Disease, you already know that artificial tears are not enough. You reapply them every 15 to 30 minutes. Your eyes still burn. Light is unbearable. Reading feels impossible. And every doctor visit ends with the same recommendation to apply more drops.
There is a better solution. Scleral lenses do not just add moisture to the eye, they replace the tear film entirely, providing all-day hydration, physical protection, and dramatically improved vision from the moment you insert them in the morning until you remove them at night.
This guide explains exactly how scleral lenses work for GVHD, what the clinical research shows, and whether you may be a candidate, including how to access this treatment right here in Michigan.
What Is Graft vs. Host Disease (GVHD)?
Graft vs. Host Disease occurs when donated stem cells or bone marrow from a transplant begin attacking the recipient’s own body, because the new immune system recognizes the host’s tissues as foreign. While GVHD can affect multiple organ systems, the eyes are among the most commonly and severely affected.
Ocular GVHD is far more common than most patients are told. Research shows it develops in 60 to 90 percent of patients following allogeneic stem cell transplantation, making it one of the most significant long-term complications of the procedure.
Ocular GVHD takes two forms. Acute GVHD typically appears within the first 100 days after transplant with sudden inflammation and rapid symptom onset. Chronic GVHD develops more gradually, sometimes months or years after transplant, and can persist indefinitely, causing progressive damage to the ocular surface if left undertreated.
How GVHD Destroys the Eye’s Surface?

To understand why scleral lenses work so well, it helps to understand exactly what GVHD does to the eye.
Goblet cell destruction
The conjunctiva, the tissue lining the inner eyelid and eye surface, contains goblet cells that produce the mucin layer of the tear film. GVHD-driven inflammation destroys these cells, causing the tear film to collapse and the corneal surface to dry out rapidly between blinks.
Lacrimal gland scarring
The lacrimal glands responsible for producing aqueous tears become infiltrated and scarred by donor immune cells, dramatically reducing or eliminating tear production. This is why preservative-free artificial tears provide only minutes of relief, there is simply nothing left to sustain a natural tear film.
Inflammatory cytokine toxicity
The ocular surface becomes bathed in inflammatory cytokines released by the attacking immune cells. These cytokines directly damage corneal epithelial cells, causing punctate erosions, corneal thinning, and in severe cases, corneal ulceration or perforation.
Meibomian gland dysfunction
The oil-producing meibomian glands in the eyelid margins also become inflamed and dysfunctional, accelerating tear evaporation and worsening the dry eye cycle.
The result is a vicious cycle: inflammation destroys tear production, the unprotected corneal surface becomes further inflamed, which drives more immune cell activity, causing more destruction.
Why Artificial Tears Fail GVHD Patients
Standard treatments include artificial tears, lubricating ointments, cyclosporine drops, steroid eye drops which address symptoms temporarily but cannot break this cycle. Artificial tears evaporate within minutes on a compromised ocular surface. Preservative-free drops used more than once per hour represent a significant burden on daily life and still leave the corneal surface exposed to inflammatory cytokines and mechanical friction from blinking.
Even autologous serum eye drops which is a more advanced option also require frequent application and provide no physical barrier against the environment.
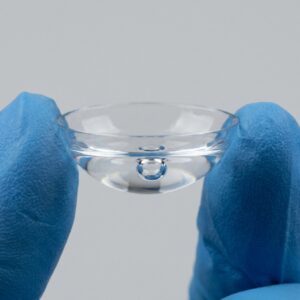
What Are Scleral Lenses and Why Are They Different?
Scleral lenses are large-diameter gas-permeable contact lenses that vault entirely over the cornea without touching it, resting instead on the white sclera of the eye. The space between the lens and the cornea is filled with sterile preservative-free saline solution before insertion.
This creates three things simultaneously that no eye drop can replicate:
A constant fluid reservoir: The saline-filled chamber bathes the cornea in moisture throughout the entire wearing period, typically 12 to 16 hours per day. There is no evaporation, no blinking interruption, no dry period between applications.
A physical barrier against cytokines and the environment: The sealed lens prevents inflammatory cytokines from reaching the corneal surface and shields the eye from wind, dust, air conditioning, and other environmental triggers that worsen GVHD symptoms.
A perfectly smooth optical surface: Even when GVHD has caused corneal scarring or irregularities, the smooth front surface of the scleral lens restores clear, sharp vision that glasses and soft lenses cannot achieve on a damaged cornea.
PROSE: The Medical-Grade Version of Scleral Lens Therapy

For the most severe cases of ocular GVHD, a specialized category of scleral lens therapy called PROSE, Prosthetic Replacement of the Ocular Surface Ecosystem is available. PROSE devices are custom-designed prosthetic lenses built to the precise contour of each individual eye using advanced scanning and impression-based techniques.
PROSE is recognized by the American Academy of Ophthalmology as a therapeutic intervention for severe ocular surface disease. Unlike standard scleral lenses, PROSE devices are designed specifically to optimize the ocular surface environment for healing, not just vision correction. It makes them particularly valuable for GVHD patients with active corneal damage or persistent epithelial breakdown.
What Does the Clinical Research Show?
The evidence supporting scleral lenses for ocular GVHD is substantial and growing.
A study conducted by the Fred Hutchinson Cancer Research Center found that 76% of GVHD patients reported significant success with scleral lens treatment. A remarkable result given that these were patients who had already failed conventional therapies.
A 2008 study of patients with ocular surface disease was conducted, including many with GVHD-related . The study found a 73% reduction in ocular pain following scleral lens fitting. Patients also reported significant improvements in their ability to perform daily activities.
A 2009 survey conducted by the Boston Foundation for Sight involved 51 GVHD patients. Most of the participants reported going from applying eye drops every 15 minutes to needing them only a few times per day after starting scleral lens wear. Patients consistently described this change as life-changing.
Research published in Bone Marrow Transplant evaluated scleral lenses for severe chronic GVHD-related keratoconjunctivitis sicca. The study confirmed both safety and effectiveness. Patients showed measurable improvement in ocular surface health markers and reported subjective comfort gains.
Scleral Lenses Compared to Artificial Tears in Ocular GVHD Treatment
| Feature | Artificial Tears / Drops | Scleral Lenses |
|---|---|---|
| Duration of relief | Minutes — evaporates rapidly | All day — constant hydration for 12–16 hours |
| Corneal protection | None — blink friction continues | Complete — lens acts as a physical shield |
| Cytokine barrier | None | Yes — sealed fluid chamber blocks inflammatory proteins |
| Environmental defense | None | High — seals out wind, dust, and air conditioning |
| Visual surface quality | Temporary blur then dryness | Smooth stable optical surface all day |
| Daily burden | 10–20+ applications per day | Once — insert in the morning, remove at night |
| Healing potential | Symptomatic only | Active — reduces inflammatory exposure to corneal surface |
Who Is a Candidate for Scleral Lenses With GVHD?
Scleral lenses are appropriate for GVHD patients who are experiencing any of the following:
- Chronic dry eye that is not adequately controlled with artificial tears or prescription drops
- Corneal damage, scarring, or epithelial erosions from GVHD
- Severe light sensitivity (photophobia) interfering with daily activity
- Blurred or distorted vision caused by an irregular or scarred corneal surface
- Significant quality of life impairment, inability to read, drive, use screens, or work
- Patients using eye drops more than once per hour who are not achieving adequate relief
There is no requirement to have failed every other treatment first. Many specialists now recommend scleral lens evaluation earlier in the course of ocular GVHD rather than as a last resort, given the evidence for their effectiveness and the potential to reduce further corneal damage.
Daily Life With Scleral Lenses: What GVHD Patients Actually Experience
The most common feedback from GVHD patients after scleral lens fitting is simply: “I got my life back.”
Patients who previously could not read for more than a few minutes, could not tolerate light, or could not drive describe being able to return to these activities within weeks of fitting. The reduction in eye drop frequency alone from dozens of applications per day to just a few, removes a constant disruption that has a profound impact on the ability to work, care for family, and engage socially.
The learning curve for insertion and removal is real, particularly given that GVHD patients often have heightened eye sensitivity and may never have worn contact lenses. However, with dedicated training from an experienced specialist, the vast majority of patients master the technique within a few sessions. Your specialist will provide insertion and removal tools, a travel case, and as many training sessions as you need.
Insurance and Cost for GVHD Patients
Because scleral lenses are prescribed as a medical device for a systemic disease, not as a cosmetic vision correction aid. They are often covered under medical insurance rather than vision insurance for GVHD patients. This is a critical distinction that can significantly reduce out-of-pocket costs.
Your specialist’s office will submit using medical necessity documentation and the appropriate billing codes for ocular surface disease management. We strongly encourage GVHD patients to ask about medical insurance billing specifically, as many patients who initially assume they are not covered discover they qualify when the correct documentation is submitted.
Scleral Lens Fitting for GVHD in Michigan
If you are in Metro Detroit, Troy, Birmingham, Oakland County, or surrounding communities, and are managing ocular GVHD, Michigan Contact Lens specializes in scleral lens fitting for complex ocular surface disease including GVHD.
We understand that GVHD patients have already been through an extraordinary amount. Our fitting process is designed to be thorough, unhurried, and focused on your comfort at every step.
Schedule a scleral lens consultation for GVHD →
Frequently Asked Question
Can I wear scleral lenses if I have extreme eye sensitivity from GVHD?
Yes! and in fact scleral lenses are often better tolerated by patients with severe ocular sensitivity than standard contact lenses. Because the lens vaults over the cornea and rests on the much less sensitive sclera, there is no lens-to-cornea contact and no “tickling” sensation from lens movement. Most patients with severe sensitivity are surprised by how comfortable scleral lenses feel compared to what they expected.
What happens if my GVHD flares while I am wearing the lenses?
During a flare, the priority shifts to managing the underlying inflammation with your medical team. Scleral lenses can typically still be worn during mild to moderate flares and may actually help protect the corneal surface during increased inflammatory activity. For severe flares involving active corneal ulceration, your eye care provider will advise temporary discontinuation until the surface has stabilized.
Can I get scleral lenses if I have never worn contact lenses before?
Absolutely. Prior contact lens experience is not required. Most GVHD patients receiving scleral lenses are new to contact lens wear. The insertion technique is different from standard soft lenses and requires more steps, but with proper training it becomes routine for the vast majority of patients within a few weeks.
How long do scleral lenses last for GVHD patients?
Typically 1 to 2 years with proper care and daily cleaning. GVHD patients may find their lens parameters need updating more frequently than other patients if their corneal shape changes as the disease progresses — regular follow-up appointments allow your specialist to monitor fit and adjust as needed.
Can scleral lenses help with night vision and light sensitivity caused by GVHD?
Yes. The stable smooth optical surface provided by the scleral lens significantly reduces the glare, halos, and light sensitivity that GVHD patients commonly experience. Many patients report that light sensitivity — one of the most debilitating symptoms — improves dramatically within the first days of wear.
Will scleral lenses cure my GVHD?
Scleral lenses do not treat the underlying immune condition — that remains the responsibility of your transplant and hematology team. What they do is protect the ocular surface from ongoing damage, provide the hydration and barrier function the eye can no longer produce on its own, and allow patients to live and function at a level that drops and ointments alone cannot achieve.