You started the morning with a crystal-clear vision. By mid-afternoon, everything looks hazy like someone smeared the inside of your lenses. You blink repeatedly. It does not help. You are not imagining it, and it is not a sign your lenses are failing.
Scleral lens fogging affects between 26% and 46% of scleral lens wearers, which makes it one of the most common complaints in specialty lens wear. The good news is that once you correctly identify which type of fogging you have, there are highly effective solutions. The bad news is that treating the wrong type with the wrong fix does nothing and can occasionally make things worse.
This guide explains the two distinct types of scleral lens fogging, what causes each one, and exactly what to do about them.
The Two Types of Fogging You Should Understand
Most articles about scleral lens fogging treat it as a single problem. It is not. There are two separate fogging locations. One is anterior surface fogging on the front of the lens, and the other is post-lens tear reservoir fogging underneath the lens and they require completely different solutions. Applying the wrong fix wastes time and money and leaves you still struggling.
Here is how to tell them apart at a glance:
| Feature | Mid-Day Fogging (MDF) | Surface Non-Wetting |
| Location | Behind the lens, in the fluid reservoir | Front surface of the lens |
| Appearance | Milky, cloudy, like diluted fog | Smudgy, oily, like grease on glass |
| When it appears | Gradually worsens through the day | Often visible shortly after insertion or after blinking |
| Blinking effect | Little to no improvement | Temporarily clears then returns |
| Primary cause | Debris/particles entering the reservoir | Lipids, oils, or poor lens wettability |
| Only reliable fix | Remove, rinse, reinsert with fresh saline | Approved wetting drops or surface cleaning |
The Role of the Reservoir in Mid-Day Fogging
Mid-Day Fogging is commonly abbreviated MDF in clinical literature as the most frequently reported type of scleral lens fogging. It occurs when particles accumulate in the tear reservoir between the posterior surface of the lens and the front of the eye during wear, causing symptoms of blurred, cloudy vision that typically worsen as the day progresses.
When you look through a lens experiencing MDF, the vision has a milky or washed-out quality as if looking through frosted glass. It does not fluctuate much with blinking because the problem is inside the sealed reservoir, not on the lens surface.
Causes Of Mid-Day Fogging
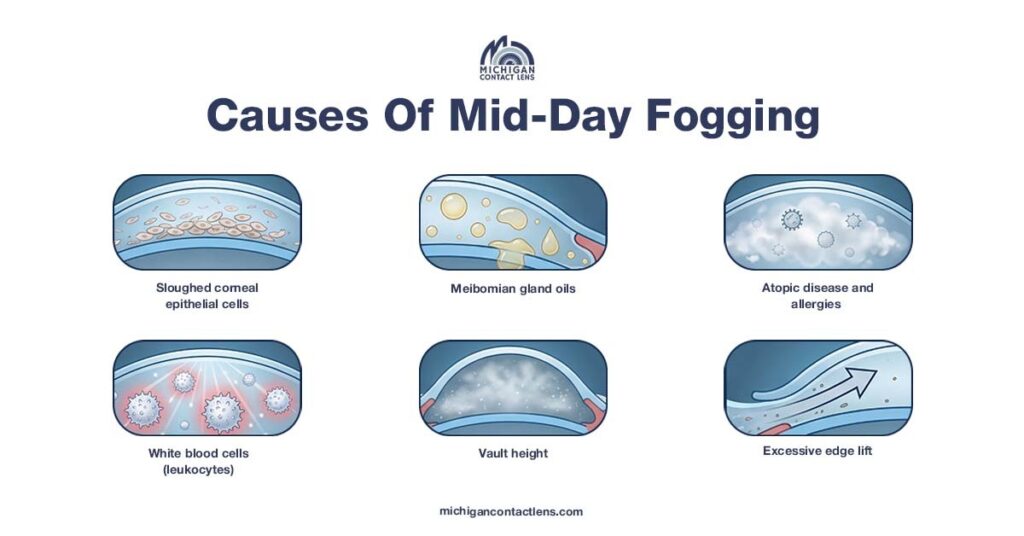
Sloughed corneal epithelial cells
The cornea naturally sheds surface cells continuously. Under a standard contact lens, this debris washes away with normal tear flow. Under a scleral lens, tear exchange is minimal compared to other lens modalities, so sloughed cells accumulate in the reservoir rather than clearing naturally.
White blood cells (leukocytes)
Research has identified leukocytes (immune cells) as a significant component of the debris found in MDF. White blood cells and tear debris accumulate in the tear fluid between the cornea and the lens, scattering light and causing hazy, cloudy vision. Their presence suggests that underlying inflammation, whether from the eye condition itself or from the lens fit, is a key driver of MDF.
Meibomian gland oils
Meibomian debris occurs when the oils from the tear film find their way under the lens and appear as semi-transparent droplets floating in the reservoir. Patients with Meibomian Gland Dysfunction (MGD) or blepharitis are significantly more prone to this type of fogging.
Excessive edge lift
If there is too much peripheral edge lift, excessive tear flow enters the reservoir, allowing debris to accumulate more rapidly. This is a fit issue that requires a lens adjustment by your specialist, not a cleaning change.
Atopic disease and allergies
Atopic disease is associated with immune responses to common allergens, which can produce a diluted milk-like fog in the lens fluid reservoir. Patients with seasonal allergies or systemic inflammatory conditions are more susceptible.
Vault height
Patients with greater than average lens vault — common in advanced keratoconus have a larger reservoir chamber with more room for particulate to build up, making MDF more likely.
What Actually Fixes MDF?
The only 100% reliable immediate fix is removal, rinse, and reinsertion with fresh saline. No drop, no blink technique, and no surface wipe will clear debris that is already inside the reservoir. Once the vision goes milky, the lens must come out.
For the prevention and reduction of MDF frequency
The saline cocktail
Adding a thicker preservative-free artificial tear, such as Refresh Celluvisc, to the bowl of the lens before filling with saline can help increase reservoir viscosity and reduce debris accumulation. Some patients use one vial to fill the lens, topping off with saline, while others develop a personal ratio that works for their tear chemistry.
Critical safety note
Always use preservative-free saline to fill your scleral lenses. Never use tap water, distilled water, or homemade saline. Tap water contains Acanthamoeba — a microorganism that can cause a severe, sight-threatening corneal infection. This is non-negotiable.
Approved reservoir solutions
Products specifically formulated for scleral lens use — such as ScleralFil, Nutrifill, and Lacripure are designed for reservoir filling and are preservative-free. Ask your specialist which they recommend for your specific situation.
Treat underlying MGD and blepharitis
If meibomian oil is the primary debris source, treating the root cause with warm compresses, lid scrubs, and eyelid hygiene can significantly reduce how often MDF occurs. Your specialist may recommend a formal dry eye or blepharitis treatment protocol alongside your lens wear.
Return for a fit evaluation
If MDF is occurring within the first 2–3 hours of wear, or happens every single day without fail, it is almost always a fit issue, excessive edge lift, too much vault, or lens movement during blinking. A loose-fitting lens acts as a pump, drawing debris under the lens very quickly. This is not something you can solve at home; it requires a lens modification appointment.
Surface Non-Wetting and the Front Surface Issue
Surface non-wetting is sometimes called anterior surface fogging, which looks completely different from MDF. Rather than a milky blur, it presents as an oily, smudgy appearance on the front of the lens, just like a fingerprint on glass. Front surface fogging looks like oil droplets on water and can often be seen quickly after a blink, with the number of droplets increasing the longer the eye remains open.
What Causes It
Poor lens wettability
The wettability of a contact lens, how easily liquid spreads across its surface, is a key factor in front surface fogging. A small wetting angle means tears spread smoothly across the lens; a large wetting angle means they bead up and cause smearing. Gas-permeable lens materials are naturally hydrophobic, meaning they repel water rather than welcoming it which is why wettability treatments exist.
Excessive lipids from eyelid disease
Conditions including MGD, ocular rosacea, blepharitis, Sjögren’s syndrome, and graft-versus-host disease all cause excess lipid production from the eyelid margins. These oils coat the front of the lens and create a hydrophobic film that tears cannot penetrate cleanly.
Oil-based cosmetics and skincare
External sources such as oil-based lotions, makeup, and hand soaps with moisturizing agents are a common and entirely preventable cause of front surface fogging. Even applying face cream before inserting lenses, if the residue reaches the lens is enough to trigger surface non-wetting.
GPC (Giant Papillary Conjunctivitis)
GPC is an inflammatory reaction that occurs in up to 15% of hard lens wearers, likely caused by the lens edge rubbing the conjunctiva. It produces increased mucus production that coats the front of the lens.
Incomplete blinking
Many scleral lens wearers, especially those on screens for extended periods, often blink incompletely, leaving the eyelid partially open. This leaves the upper portion of the lens exposed and unrefreshed, allowing deposits to accumulate on areas the tear film never reaches. Practicing full, deliberate blinks, consciously closing the eye completely can make a measurable difference.
What Actually Fixes Surface Non-Wetting?
Switch to oil-free cosmetics. This is the single most impactful lifestyle change for patients whose surface fogging began around the same time they started a new skincare routine or switched makeup brands. Look specifically for products labeled oil-free and lens-safe. Apply all face creams, moisturizers, and makeup after inserting your lenses — never before.
Hydra-PEG coating. Hydra-PEG is a thin, permanently applied coating on the front lens surface that improves wettability, increases water retention, and significantly reduces deposit accumulation. It is particularly beneficial for scleral lens wearers with heavy lipid deposits or persistent surface fogging. This is applied during manufacturing — ask your specialist whether your current lenses have it and whether it is appropriate for your situation.
Peroxide-based cleaning systems. Hydrogen peroxide systems such as ClearCare provide a deeper clean than multipurpose solutions and are highly effective at breaking down lipid and protein deposits on the lens surface. If you are currently using a multipurpose solution and struggling with surface fogging, switching to a peroxide system is often the first recommendation.
Plasma treatment awareness. Scleral lenses are typically plasma-treated during manufacturing, which cleans the lens surface using ionized oxygen and significantly improves wettability. This treatment degrades over time — if your lenses are more than a year old and surface fogging has worsened, the plasma treatment may have worn off and new lenses may be indicated.
Treat eyelid disease. If MGD or blepharitis is identified as the lipid source, a formal eyelid hygiene protocol — warm compresses for 5 minutes twice daily, followed by lid massage and a gentle hypochlorous acid lid cleanser — can dramatically reduce the oils reaching the front of the lens.
One Type of Fogging Requires Urgent Attention: Corneal Edema
Not all hazy vision in scleral lens wearers is fogging. If a patient reports hazy vision and sees rainbows around lights, it is critical to evaluate the cornea for microcystic edema — also known as Sattler’s veil. If this is present, lens removal and reapplication will not resolve symptoms. Instead, the patient needs medical management, and scleral lens wear may need to be discontinued or significantly limited.
If your vision haziness is accompanied by rainbow halos around lights, remove your lenses and contact your eye care specialist promptly. This is distinct from standard MDF and should not be self-managed.
What You Should Never Use for Scleral Lens Fogging?

Commercial anti-fog sprays. Products marketed for glasses, ski goggles, or bathroom mirrors are toxic to the eye. They are not formulated for ocular use and should never contact a lens that goes in your eye. There is no over-the-counter anti-fog spray that is safe for scleral lenses.
Tap water in any form. Never rinse, fill, or store scleral lenses with tap water. Even brief exposure introduces the risk of Acanthamoeba keratitis, a painful, potentially blinding infection that is extremely difficult to treat.
Preserved saline or multi-purpose solution as a reservoir filler. Preservatives that are safe for brief soft lens contact are not appropriate for the prolonged reservoir contact of scleral lens wear. Always use preservative-free saline specifically approved for scleral lens filling.
Daily Habits That Prevent Both Types of Fogging
- Wash hands with a fragrance-free, oil-free soap and rinse thoroughly before handling lenses, moisturizing hand soaps are a major but overlooked source of surface contamination
- Apply all skincare and makeup after inserting lenses, never before
- Clean lenses every single day with your recommended cleaner — skipping days allows deposit buildup that compounds rapidly
- Practice full blinks, consciously close your eyes completely several times per hour, particularly during screen use
- Store lenses overnight in multi-purpose solution (not saline) — saline does not disinfect
- Schedule regular follow-up appointments — fit changes from corneal shape progression are a leading cause of suddenly worsening MDF that patients often try to manage with cleaning changes instead
When to See Your Specialist About Fogging
Return for an appointment when:
- MDF is occurring within 2 hours of insertion every day
- You are removing and reinserting lenses more than once per day to manage fogging
- Surface fogging appears immediately after insertion and does not respond to cleaning changes
- You notice rainbow halos around lights alongside hazy vision
- Fogging is accompanied by discomfort, redness, or increased light sensitivity
- The problem has significantly worsened without any change in your routine
Fogging that has a sudden onset after months of clear wear usually signals a fit change, a new systemic condition, a change in tear chemistry, or a new product in your routine — all of which your specialist can identify and address quickly.
Scleral Lens Fogging Help in Michigan
If you are managing persistent scleral lens fogging in the Metro Detroit area, Troy, Birmingham, or Oakland County. Michigan Contact Lens specializes in complex scleral lens troubleshooting. Whether the issue is fit, tear chemistry, lens surface treatment, or underlying eyelid disease, we can identify the specific cause and adjust your management plan.
Schedule a scleral lens appointment →
Frequently Asked Questions
Why do my scleral lenses fog up after only 2 to 3 hours?
Early-onset MDF almost always points to a fit issue — most commonly excessive edge lift or too much vault. This creates a large reservoir that fills with debris quickly. It requires a lens modification, not a cleaning change.
Can I use rewetting drops to clear fogging?
For surface non-wetting, preservative-free drops applied over the lens can temporarily improve clarity. For reservoir MDF, drops applied to the front cannot reach debris inside. Removal and reinsertion are the only solutions.
Is it safe to remove and reinsert my lenses multiple times a day?
Yes, with proper technique and preservative-free saline. The main risks are contamination from improper handling and Acanthamoeba from water exposure. Both are prevented by strict hygiene and the use of only approved preservative-free saline.
Why did my fogging suddenly worsen after months of no problems?
Sudden onset usually means one of four things: your corneal shape has changed, you introduced a new skincare or cosmetic product, your underlying dry eye or eyelid condition has progressed, or your lens surface treatment has degraded. Your specialist can identify which within a single appointment.
Does Hydra-PEG wear off?
The coating bonds permanently to the lens material but can be damaged by incompatible cleaning products. Always confirm your solution is Hydra-PEG compatible. Peroxide systems are generally safe, but some multipurpose solutions degrade the coating over time.
Can blepharitis cause scleral lens fogging?
Yes. Blepharitis is one of the most common underlying drivers of both MDF and surface non-wetting. Treating it with a consistent eyelid hygiene protocol often reduces fogging significantly without any lens change needed.